
 TAM (Treatments and Medicines) NHS Highland
TAM (Treatments and Medicines) NHS Highland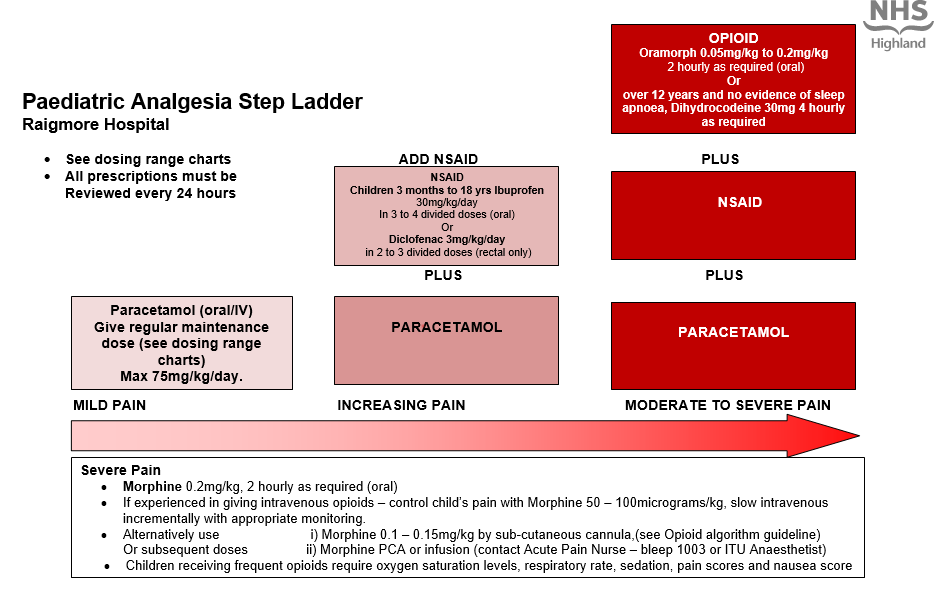
Analgesia (Paediatric Guidelines)

Warning
- Use the oral route whenever possible.
- Verbal consent should be obtained from the child and/or parent if the rectal route is to be used. Also if the child has had bowel surgery, check with the surgeon that the rectal route may be used.
- Prescriptions for regular opioids should be reviewed by anaesthetic/pain team / medical staff daily.
- When changing from one route of administration to another, use “step-over” doses (equipotent) until you can assess the effect. Later you can change to “step-down” drugs (less potent) when appropriate.
- Give Paracetamol and NSAID’s regularly as prescribed and opioids as required. A multi-modal approach improves pain relief and reduces the child’s opioid requirement.
- Do not prescribe compound analgesics for children. eg. Co-codamol.
- All prescriptions must be reviewed every 24 hours
Paracetamol dose in children - oral route
- Paracetamol can be administered by the oral routeREGULARLYfor the relief of mild to moderate pain and as an adjunct to stronger analgesics in severe pain.
- If the patient has not received any paracetamol in the preceding 24 hours, a loading dose of 20mg/kg (prescribed on the ‘ONCE ONLY’ section of the drug kardex) may be used if necessary, followed by the usual dose.NB this is included in the patient’s total daily dose.
- Do not exceed 1g in a single dose or 4g in 24 hours.
- All Children should be dosed by weight rather than age. If the weight is unknown then follow the dosing by age in the BNF for Children.
| Age | Dose | Interval | MAXIMUM DAILY DOSE |
Pre-term neonate 28-32 weeks corrected gestational age | 10mg/kg | 8 hourly up to three times daily | 30mg/kg/day |
Neonate over 32 weeks corrected gestational age | 15mg/kg | 6 hourly up to four times daily | 60mg/kg/day |
1 month to 18 years | 15mg/kg up to a max of 1g | 4 hourly up to four times daily | 75mg/kg/day |
Paracetamol dose in children - rectal route
- When the oral and the IV routes are not available, Paracetamol can be administered by the rectal route but dosing can be complex as bioavailability is very variable.
- If the patient has not received any paracetamol in the preceding 24 hours, a loading dose of 30mg/kg may be given followed by the usual dose
- Child 1 month to 18 years 15- 20mg/kg per dose
- Suppositories should not be halved.Doses are adjusted according to the suppository strength available.
- Maximum of 4 doses may be given in 24 hours.
- The maximum daily dose is 75mg/kg/day, up to max of 4g daily (for 5 to 12 years as per BNFc).
| Age | Dose | Interval | MAXIMUM DAILY DOSE |
1 to 3 months | 60mg | Every 4 hours | 75mg/kg/day |
3 to 12 months | 60 to 120mg | Every 4 hours | 4 doses in 24 hours (or 75mg/kg/day) |
1 to 5 years | 120 to 240mg | Every 4 hours | 4 doses in 24 hours (or 75mg/kg/day) |
| 5 to 12 years | 240mg to 500mg | Every 4 hours | 4 doses in 24 hours (or 75mg/kg/day. Maximum 4g daily) |
12 to 18 years | 12 to 18 years | Every 4 hours | 4 doses in 24 hours |
Paracetamol dose in children - IV route
- When the oral route of administration is unavailable, IV preparations of paracetamol should be considered.
- IV paracetamol is no more potent or effective than oral paracetamol but dosing is reduced in certain circumstances due to a greater potential for toxicity.
- All IV doses should be administered as a slow IV infusion over aminimum of 15 minutesto avoid hypotension.
- Do not exceed 1g as a single dose or 4g in a 24 hour period.
- Consideration should be made to decreasing the maximal dosing further in the presence of hepatic impairment, malnutrition, dehydration and muscle disorders.
| Patient | Dose | Interval | MAXIMUM DAILY DOSE |
Pre-term Neonate over 32 weeks corrected gestational age | 7.5 mg/kg | 8 hourly | 22.5mg/kg/day |
Term Neonate | 10 mg/kg | 4 hourly, up to three times daily | 30mg/kg/day |
Child under 10kg | 10 mg/kg | 4 hourly, up to three times daily | 30mg/kg/day |
Child 10 to 50kg | 15 mg/kg | 4 hourly, up to four times daily | 60mg/kg/day |
Child over 50kg | 1g | 4 hourly, up to four times daily | 4g/day |
NSAIDs provide useful analgesia especially in Musculoskeletal pain, Inflammatory pain and Bone pain
NSAIDs may have adverse effects so care should be taken when determining if NSAIDs are suitable for patients and when prescribing/ reviewing therapy. Please check through the list below before prescribing NSAIDs.
Non-steroidal anti-inflammatory Dosing in children
IBUPROFENcan be administered by theoral routeevery 6 to 8 hours.
The dose is 5 mg/kg up to 30 mg/kg/day.
Cautions – see list on NSAID flow chart
| Age |
Standard Dose |
Standard Interval
|
Maximum Dose |
|
1 to 3 months |
5mg/kg |
6 to 8 hourly |
up to four times daily |
|
3 months to 18 years |
5mg/kg up to 400mg |
6 to 8 hourly, up to three times daily |
7.5mg/kg as a single dose up to 30mg/kg/day |
PREPARATIONS AVAILABLE:
Suspension: 100mg/5ml
Tablets: 200mg and 400mg
DICLOFENAC
If the oral route is not available then DICLOFENAC can be administered by the rectal route.
| AGE | DOSE | INTERVAL | COMMENT |
|
6 months to 18 years |
0.3 to 1mg/kg up to 50 mg |
8 hourly | The dose must be adjusted according to the suppository strength available |
PREPARATIONS AVAILABLE:
Suppositories: 12.5mg, 25mg, 50mg
Oral Opioid Doses
Age | Dose | Interval |
6 months - 17 years | Oramorph | Up to 2 hourly |
Over 12 years | Dihydrocodeine | Up to 4 hourly |
Oral opioids have the same side effects as parenteral opioids and the following need to be carried out:
Routine post-operative observations: pulse, oxygen saturation levels, respiratory rate, pain score, sedation score and nausea score should be recorded on the observation chart.
- Assess effects half an hour after each administration of opioid
Oxygen saturation levels less than 94% on air (with no other known cause)
- Administer oxygen by facemask, commence with 4 litres per minute and titrate until sats >95% and ensure a clear airway.
- Stay with the child and monitor respiratory rate, sedation and oxygen saturation levels continuously.
- Contact the On call/duty anaesthetist for further advice.
- Assess for other causes of hypoxia/sedation.
- Reduce subsequent dose of opioid by half and assess if the child's pain can be managed with regular paracetamol and/or NSAIDS (oral/rectal).
Respiratory depression
Oral opioids have the same side effects as parenteral opioids and the following need to be carried out:
| Age | Breaths per minute |
| Less than 6 months | below 20 breaths per minute |
| 6 months to 2 years | below 16 breaths per minute |
| 2 years to 7 years | below 14 breaths per minute |
| 8 years and over | below 10 breaths per minute |
- Ensure a clear airway and administer oxygen 4 litres per minute via face mask and titrate until sats >95%.
- Stay with the child and monitor the respiratory rate, sedation and oxygen saturation levels continuously.
- Contact the paediatrician and On Call/Duty anaesthetist for further advice.
- Assess for other causes.
- Reduce subsequent doses of opioids by half and assess if the child’s pain can be managed with paracetamol and /or NSAIDS.
Severe respiratory depression
| Age | Breaths per minute |
| Less than 6 months | below 18 breaths per minute |
| 6 months to 2 years | below 14 breaths per minute |
| 2 years to 7 years | below 12 breaths per minute |
| 8 years and over | below 8 breaths per minute |
- Ensure a clear airway and administer oxygen face mask, commence with 4 litres per minute and titrate until sats >95%.
- Contact the paediatrician and On Call/Duty anaesthetist to review urgently.
- Administer Naloxone (10 micrograms/kg IV in increments. e.g for a 30kg child the maximum dose of Naloxone is 300mcg. Give ¼ of the dose and repeat after 1 minute intervals if there is an inadequate response until the maximum dose of Naloxone has been given. A Naloxone infusion may be required.
- If the response to Naloxone is inadequate then consider other causes.
- The child must be nursed in the high dependency area until opioids are no longer required. Continuous pulse oximetry must be used.
- Reduce subsequent doses of opioids by half and assess if the child’s pain can be managed with paracetamol and /or NSAIDS.
Side effect management
Constipation
- Laxatives should be prescribed for any child receiving regular opioids.
- Ensure a high fibre diet and adequate fluid intake
- Assess for other causes
Nausea and Vomiting
- If a child complains of nausea or is vomiting please give the prescribed anti-emetic
- See paediatric post operative nausea and vomiting (PONV) guidelines
- Children receiving regular opioids may require regular prophylactic anti-emetics
- If problem continues despite treatment as per guidelines consider iv fluid therapy to maintain hydration
Itching
- Assess cause – it may not be the opioid- rash with dressings etc
- Prescribe antihistamine as required – Chlorphenamine Doses:
Child 2 – 6 years 1mg, every 4-6 hours. Max 6 mg daily.
6 – 12 years 2mg every 4-6 hours. Max 12mg daily.
12 – 18 years 4mg every 4-6 hours. Max 24mg daily
Use Opioids with caution in the following groups of children as they may need a reduced dose and longer dosing interval
- Children with moderate to severe renal impairment.
- Children with moderate to severe liver impairment.
- Children with sleep apnoea, upper airway abnormalities or those at risk of upper airway obstruction.
- Children with severe neurological disorders
Oxycodone oral solution
Oxycodone oral solution (1mg/ml) can be used as an alternative strong opioid when morphine is contraindicated. This is not a stock medication and must be ordered in advance through pharmacy. The dosing regimes in the BNFc are for moderate to severe oncological pain and a 30-50% dose reduction may be more appropriate for treatment of moderate post-operative pain.
- Morphine 0.2mg/kg, 2 hourly as required (oral)
- If experienced in giving intravenous opioids – control child’s pain with Morphine 50 – 100mcg/kg, slow intravenous incrementally with appropriate monitoring.
- Alternatively use i) Morphine 0.1 – 0.15mg/kg by sub-cutaneous cannula, (see Opioid algorithm guideline)
- Or subsequent doses ii) Morphine PCA or infusion (contact Acute Pain Nurse – bleep 1003 or On call/Duty Anaesthetist)
- Children receiving frequent opioids require oxygen saturation levels, respiratory rate, sedation, pain scores and nausea score