
 Optimising glycaemic control in people with type 1 diabetes (SIGN 170)
Optimising glycaemic control in people with type 1 diabetes (SIGN 170)

The AGP may be used to guide glycaemic management of people with diabetes. Assessment should be based on a number of further measures, for example Glucose Management Indicator (GMI), Time in Range (TIR), frequency of severe hypoglycaemia.
When using the AGP, a systematic approach to interpreting CGM data is recommended:
- Review the overall glycaemic status (eg, GMI, average glucose)
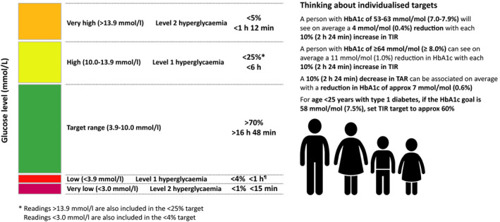
- Check Time Below Range (TBR), TIR, and Time Above Range (TAR) statistics, focusing on hypoglycaemia (TBR) first. If the TBR statistics are above the cutpoint for the clinical scenario (ie, for most people with type 1 diabetes >4% <3.9 mmol/L; >1% <3.0 mmol/L), the visit should focus on this issue. Otherwise, move on to the TIR and TAR statistics.
- Review the 24-hour glucose profile to identify the time(s) and magnitude(s) of the problem identified.
- Review treatment regimen and adjust as needed.
The two metrics, %TIR and %TBR, should be used as a starting point for the assessment of glycaemic control and as the basis for therapy and lifestyle adjustment. Particular emphasis on reducing %TBR is warranted when the percentages of CGM values falling below 3.0 mmol/L or 3.9 mmol/L are close to or exceed targets.
Continuous glucose monitoring metrics derived from continuous glucose monitor use over the most recent 14 days (or longer for patients with more glycaemic variability), including time in range (3.9–10 mmol/L), time below target (<3.9 mmol/L and <3.0 mmol/L), and time above target (>10 mmol/L), are recommended to be used in conjunction with HbA1c whenever possible.
Ambulatory Glucose Profile (AGP) is a report summarising CGM data over multiple days of wear and is available from all CGM devices and the linked reporting tools. These reports allow a standardised summary of key information consisting of some or all of the following: data completeness, glucose level statistics (eg, hypoglycaemia, hyperglycaemia and TIR), glucose profile based on a “summary day” (also named the AGP), glucose management indicator (GMI) and daily glucose profiles.
A UK Best Practice Guide on Glucose Metrics can be found at Time in range: A best practice guide for UK diabetes healthcare professionals in the context of the COVID‐19 global pandemic. We support the guidance that ‘%TIR should be used in conjunction with AGP data for a fuller picture of glycaemic health and as a basis for managing therapy and making treatment decisions’. It is important that clinicians appreciate that %TIR is not a surrogate for HbA1c and has a clinical utility that is different from HbA1c, since %TIR reflects the combined influence of glucose exposure and the degree of glycaemic variability.
Source: Wilmot EG, Lumb A, Hammond P, Murphy HR, Scott E, Gibb FW, et al. Time in range: A best practice guide for UK diabetes healthcare professionals in the context of the COVID-19 global pandemic. Diabet Med. 2021 Jan;38(1):e14433. https://doi.org/10.1111/dme.14433
The review of AGP data in the clinic should be guided by the issues brought to the consultation by the person with diabetes as these will need to be dealt with before they will be ready to discuss the AGP.

